
Audio
Surgery for Femoroacetabular Impingement
What Happens at Hip Arthroscopy?
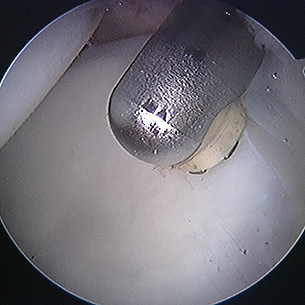
Excision of CAM impingement lesion under way using high speed burr.
Capsulotomy being undertaken with arthroscopic knife.

Repairing a torn acetabular labrum
Using a radiofrequency probe in the hip
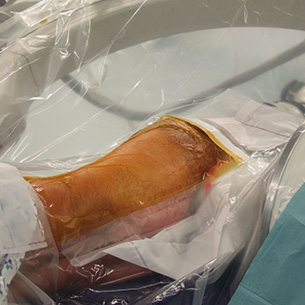
A patient prepared and positioned for a hip arthroscopy. The head is to the left and the feet to the right. We are standing at the back of the patient.
The idea of using a tubular viewing device in order to perform surgery is not new. Surgeons have been undertaking such procedures for more than one hundred years. However, some areas have proved harder than others when it comes to identifying a safe and suitable technique. The hip is most certainly one such area.
The problem has been the deep-seated nature of the hip joint and its ball-and-socket shape. One look at it is enough to agree with a Dr Burman who, in 1931, deemed hip arthroscopy impossible. However, the secret, if that is the correct word, is to understand that the hip joint is held together not only by its shape, muscles and ligaments, but also by suction.
Consequently, the hip arthroscopic surgeon will first of all pull on the leg (traction) with some form of specialist distractor in order to open up the hip a tiny amount. Once this first gap is made, it is possible to insert a needle into it and equalise the pressure inside the joint with atmospheric pressure. The moment that happens, so the hip opens up, just like magic! That is the principle, of course. Life is not always as easy as one might like, however, so gaining access to the interior of the hip joint can sometimes prove very difficult, even for the most experienced surgeons. Sometimes access is impossible.
Once the hip has opened up, an arthroscope is passed into it. This is approximately 5mm in diameter. A camera is attached to the end of the arthroscope and the image is displayed on a nearby screen. Surprisingly, it is uncommon for the surgeon to look at the patient very much at all during a hip arthroscopy. Most of the action is on the screen and it is there that the surgeon generally looks.
Once the arthroscope is in the joint, operating instruments are also inserted. These are not passed down the same portal of entry as the arthroscope but through adjacent portals. The operating instruments are of different designs but may be manual cutters, powered shavers and burrs, or radiofrequency probes. Radiofrequency is now widely used at hip arthroscopy. Lasers are less commonly used, although there was a period some years ago when laser hip arthroscopy was undertaken in a few specialist centres.
The use of traction for hip arthroscopy allows access to the area of the hip known as the central compartment. This is the area directly between the ball (femoral head) and socket (acetabulum). Here can be found the labrum, the ligamentum teres, and much of the gristle covering of the ball and socket. However, once the central compartment has been treated, the surgeon may then proceed to gain access to the peripheral compartment. This is the area outside the hip socket but still inside the hip itself and largely comprises the outer surface of the hip ball. To access the peripheral compartment does not require traction.
However, the ball is placed back in the socket and the hip is bent slightly, to about 25 degrees. This allows the soft-tissue structures on the front of the hip to relax so that a space appears between them and the front of the hip ball. It is possible to insert the arthroscope and operating instruments into this space and to undertake surgery in this area. Most hip arthroscopic procedures will involve accessing both the central and peripheral compartments at various stages during the operation.
A hip arthroscopic procedure is thus not a simple process and does take time, often longer than a total hip replacement operation. The presence of just a few tiny incisions at the end of the operation does not mean that the operation is tiny too. Much can be done with a hip arthroscope!
The Princess Grace Hospital, 30 Devonshire Street, London, W1G 6PU | Enquiries: +44 (0)207 908 3777 | Fax: +44 (0)203 752 6501
enquiries@villarbajwa.com
© Villar Bajwa Practice (2015) | Terms & Conditions